We are happy to announce that the authors of Primary Care Breakfast Club published a perspective piece in the New England Journal of Medicine on September 6, 2012. Our piece, titled "The Developing Vision of Primary Care", has received a lot of feedback from all sides. If you are interested in continuing the conversation, feel free to leave a comment.
To read the piece, visit the following link: http://www.nejm.org/doi/full/10.1056/NEJMp1204487
We hope you enjoy and would love to hear your feedback!

Saturday, October 27, 2012
Tuesday, May 1, 2012
Primary Care Spring
IBM is launching what they are calling the "Primary Care Spring." At the risk of upstaging Occupy Spring they are seeking to revolutionize the way they take care of their employees by widely promulgating the Patient Centered Medical Home (PCMH). They are certainly not the first, but they represent a growing number of large insurers that have jumped on the wagon.
In a YouTube video presentation by Dr. Paul Grundy of IBM that can be found at the above link he describes 3 trends he is seeing:
1. Cost: good comprehensive coordinated patient-centered care saves money
2. Data: we can now help physicians make better clinical decisions because we now have the data needed to do so (how could he give a presentation without mentioning "Watson"?)
3. On-line asynchronous care: medical homes succeed because they allow for on-line and asynchronous care where you don't have to see your doctor to be treated and they don't have to see you to get paid. In this new information age our children will not put up with receiving care any other way.
In short, this is nothing new but it is all coming together across the country. The government, insurers, employers, providers, and patients are all recognizing that accessible, coordinated, patient-centered care really does save money and make people healthier.
You CAN have your cake and eat it too.
-JKR
In a YouTube video presentation by Dr. Paul Grundy of IBM that can be found at the above link he describes 3 trends he is seeing:
1. Cost: good comprehensive coordinated patient-centered care saves money
2. Data: we can now help physicians make better clinical decisions because we now have the data needed to do so (how could he give a presentation without mentioning "Watson"?)
3. On-line asynchronous care: medical homes succeed because they allow for on-line and asynchronous care where you don't have to see your doctor to be treated and they don't have to see you to get paid. In this new information age our children will not put up with receiving care any other way.
In short, this is nothing new but it is all coming together across the country. The government, insurers, employers, providers, and patients are all recognizing that accessible, coordinated, patient-centered care really does save money and make people healthier.
You CAN have your cake and eat it too.
-JKR
Monday, April 30, 2012
It's the Hospitals Stupid!
Massachusetts has been leading health reform at the state level since passing far-reaching legislation in 2006 that was the blueprint for the Affordable Care Act. They are at it again. As Martyna Skowron, a colleague from Harvard School of Public Health writes, the Massachusetts House and Senate are close to releasing their versions of comprehensive payment reform legislation for the state healthcare system. What they're likely to propose may surprise you.
Much has been made of the problem of prices in our health care system. Uwe Reinhardt, back in May 2003, wrote an article in Health Affairs titled It's the Prices Stupid: Why the United States Is So Different From Other Countries. He's been writing about the issue ever since. In short, payers in the US system pay far more for the same services in absolute dollar amounts than payers in other health systems around the world.
What follows is an excerpt from the Massachusetts Attorney General's Preliminary Report on the drivers of health care costs in the state. It is titled Investigation of Health Care Cost Trends and Cost Drivers and was released last year.
Much has been made of the problem of prices in our health care system. Uwe Reinhardt, back in May 2003, wrote an article in Health Affairs titled It's the Prices Stupid: Why the United States Is So Different From Other Countries. He's been writing about the issue ever since. In short, payers in the US system pay far more for the same services in absolute dollar amounts than payers in other health systems around the world.
Why? Extending the argument one step further, as I did in this post late last year, we find ourselves at the doorstep of the hospitals who set those prices.
"We focused our investigation on contracting practices and contract prices (i.e., the prices negotiated between health insurance companies and hospitals and physicians for hospital inpatient and outpatient care, and professional services) for commercial health insurance for the period 2004 through 2008. While our investigation continues and our analysis is not final, our preliminary review has revealed serious system-wide failings in the commercial health care marketplace which, if unaddressed, imperil access to affordable, quality health care. In brief, our investigation has shown:
- Prices paid by health insurance companies to hospitals and physician groups vary significantly within the same geographic area and amongst providers offering similar levels of service.
- Price variations are not correlated to (1) quality of care, (2) the sickness or complexity of the population being served, (3) the extent to which a provider is responsible for caring for a large portion of patients on Medicare or Medicaid, or (4) whether a provider is an academic teaching or research facility. Moreover, (5) price variations are not adequately explained by differences in hospital costs of delivering similar services at similar facilities.
- Price variations are correlated to market leverage as measured by the relative market position of the hospital or provider group compared with other hospitals or provider groups within a geographic region or within a group of academic medical centers.
- Variation in total medical expenses on a per member per month basis is not correlated to the methodology used to pay for health care, with total medical expenses sometimes higher for globally paid providers than for providers paid on a fee-for- service basis.
- Price increases, not increases in utilization, caused most of the increases in health care costs during the past few years in Massachusetts.
- The commercial health care marketplace has been distorted by contracting practices that reinforce and perpetuate disparities in pricing."
Does this surprise you? In a nutshell, hospitals have been able to set high prices for their services which insurance companies must pay because hospitals possess monopolistic market share in specific health care markets. While we would hope there is more sense to the prices we pay for health care, such that we are paying more for better care, more timely care, or because we have more complex disease, this is not the case.
The question now is: what do we do about it? The free market can only help if competition is introduced into the market. Instead, hospitals have been consolidating, making the problem worse. Is it now time for the government to step in again? The Massachusetts legislature will likely unveil proposals that endorse a multi-pronged approach. The biggest prong will be encouraging global payment and setting "milestones for growth." Furthermore, they are likely to enable the state to step in if growth is not limited to these milestones. Additionally the proposal will likely include provisions to increase price transparency, ensure more competitive market behaviors, and promote further research into cost drivers and policies that encourages providers and consumers to utilize more cost-effective care.
It should be interesting and may again influence decisions made on the national stage in regards to price reform in the future.
-JKR
Monday, March 26, 2012
Supreme Court to Start Hearings on Health Reform Today
Today, the Supreme Court will begin hearings regarding the constitutionality of parts of the Affordable Care Act (ACA). The Supreme Court will hear six hours of oral arguments over the course of the next few days looking at three issues. First, they are looking at the legality of the individual mandate. Second, they will decide if this part of the law can be severed from the rest of the ACA. And three, they will hear about the constitutionality of Medicaid expansion.
Titles I and II of the ACA will reduce the number of uninsured citizens in our country through two mechanisms: required insurance by everyone and by expanding Medicaid.
Title I is the divisive individual mandate whereas every person in this country is required by law to purchase health insurance or else they face a fine. This is similar to car insurance requirements. The individual mandate, which is historically a Republican policy idea, has been controversial since the bill was passed. Economist argue that by requiring everyone to buy insurance this will broaden the risk pool thereby protecting us all financially. Additionally, by requiring health insurance, it will reduce moral hazard such that people will not seek out coverage only when they are sick or injured.
Title II expands Medicaid to cover everyone who is under 133% of the federal poverty line. It is estimated that the Medicaid expansion will result in half of the newly insured 32 million Americans.
An important aspect of the Supreme Court hearings is whether or not the ACA can stand without Titles I and/or Title II. The ACA has already benefited millions of Americans. Young adults, who make up the second largest group of uninsured Americans, are already covered. Women's health insurance premiums have been reduced equal to their male counterparts. Provisions regarding prescription drug coverage have already saved our elderly population $32 billion. Children and adults are no longer denied coverage because they have a pre-existing condition. And most importantly, as a country we have come together to reach out to our most vulnerable populations.
The hearings this week and the subsequent ruling, which is expected to come out later this spring, will be historic and will significantly impact the lives of all Americans. For the sake of our country's health and economy, I hope to see the legislation held up.
Thursday, March 22, 2012
Match Results Are In
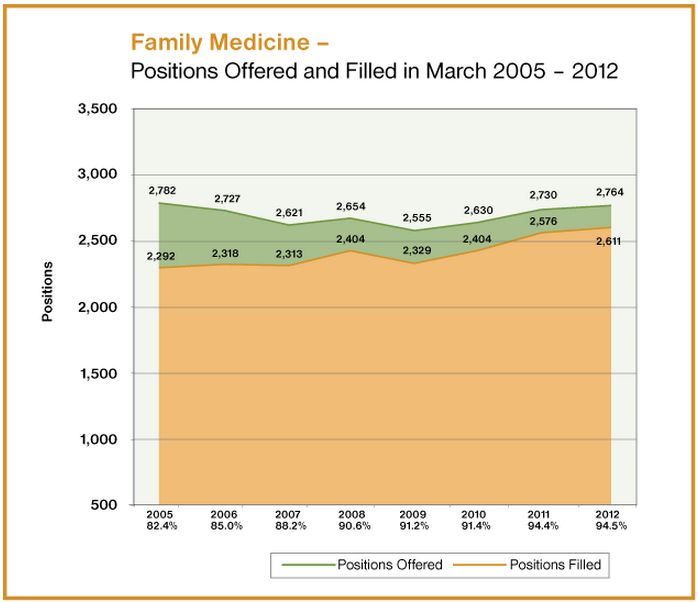 Last Friday, graduating medical students across the country received their residency match results. For the third straight year, there has been an increase in the number of students matching into family medicine. This year 94.5% of all family medicine spots were filled and the total number of U.S. grads entering the field in 2012 is 1,335. This is an increase in 18 seniors compared to 2011. Family Medicine added 34 new residency positions this year and 35 more total students (U.S. + non-U.S. grads) entered the field compared to 2011.
Last Friday, graduating medical students across the country received their residency match results. For the third straight year, there has been an increase in the number of students matching into family medicine. This year 94.5% of all family medicine spots were filled and the total number of U.S. grads entering the field in 2012 is 1,335. This is an increase in 18 seniors compared to 2011. Family Medicine added 34 new residency positions this year and 35 more total students (U.S. + non-U.S. grads) entered the field compared to 2011. Although the numbers are increasing, I hope to see further increases in the years to come. The rate of new family doctors is not keeping pace with demand and there needs to be a much larger bump in these numbers in 2013 and the following years in order to effectively serve the population's health needs.
Image from aafp.org
Wednesday, March 21, 2012
Duke's Primary Care Leadership Track
Future primary care providers will work in patient centered medical homes (PCMHs). This new model of care will be different than traditional practice models. Primary care physicians will work in inter-disciplinary teams, be expected to coordinate and integrate care with others in the medical neighborhood, and they will be held accountable for the quality of care provided to patients. Medical schools are responding by implementing programs and special tracks to prepare medical students to work in these innovative practice models.
One of the best examples nationally is Duke University School of Medicine's Primary Care Leadership Track (PCLT). Applicants to Duke's program apply specifically to the PCLT and this year alone they received well over a hundred applications. The PCLT works to develop students into national leaders in primary care.
The first year of medical school is largely the same in that students in the PCLT spend the majority of their time studying the basic sciences. At the end of their first year, they take their step 1 exams and immediately move into a longitudinal clerkship experience.
Students spend about 80 percent of their time in the outpatient setting alternating clinic days between medical practices. For example, every Monday a student will go to an internal medicine clinic, Tuesday she will go to her Family Med Clinic, Psychiatry on Wednesday, and Pediatrics on Thursday. This provides the students with continuity of care within each of the core disciplines and gives them a chance to follow their patients' care over the course of a year.
Students also are assigned to a panel of about 20 patients who they follow throughout the entire year. Every time one of the patients in their panel has a medical appointment, surgery, emergency department visit, or baby delivery, the student is expected to be there with the patient. This provides students with the unique insight of how patients flow through the medical system.
Within the PCLT curriculum, students go through a PCMH mini-course. The mini-course is designed to teach students the core values of primary care and PCMHs. Students are then engaging in medical practices who are working towards PCMH accreditation by taking on an innovation projects. A good example of a project is when one student worked with a clinic to meet phone call back goals. The student tracked the average length of time it took the clinic to call their patients back and then he worked with the clinic to shorten the interval. Other projects have looked at follow up rates and length of time from the point of hospital discharge, quality metrics for diabetic patients, and rate of specialist to primary care provider communication after the patient sees their specialist physician.
Engaging students in innovation projects is developing strong leadership skills and showing students the inner workings of this new model of care. Students will be ahead of their peers once they start practicing as they will have real life experience in improving practice models which are truly patient-centered.
Duke's focus on primary care is inspiring and they are setting the bar for preparing and producing future leaders in primary care medicine.
Friday, March 9, 2012
Prevention and Public Health Fund Gets Cut
On February 22, 2012, President Obama signed legislation to cut funding from the Prevention and Public Health Fund. This fund was created by the Affordable Care Act (ACA) and invested $15 billion over 10 years to prevent disease and promote wellness in our society. This was a major advancement in U.S. health policy which shifted focus on creating a healthy and productive society rather than one that only reacts to disease once patients are already ill.
Prevention and public health are frequently the first place to start enacting cuts, but this is a huge mistake. Most diseases and causes of death in the U.S. are preventable, yet we continue to turn our backs on efforts to stop disease, illness, injury, and even death before they develop. When we have an unhealthy society, this affects many sectors of our economy as sick or injured workers are not as productive as they could be. Additionally, by continuing to only invest at the end of the line, care is reactionary and costly for the patients.
I think three primary reasons explain why investments in public health and prevention are often overlooked. First, people do not understand what public health is. It is more than just responding to infectious disease outbreaks or tracking influenza strains. Public health makes sure that the food we eat is sanitary, the air we breathe is clean, and that our roads are safe to drive on. Nearly every facet of our lives places us in danger, but public health professionals seek to minimize risks. Most public health interventions are inconspicuous and out of the public eye, so it is not surprising that political will for public health initiatives is minimal.
Second, prevention does not make anyone any money. Health care is big business these days and bottom lines for those in the health industry only decrease when people are healthy. Money comes at the end of the line: surgery for the diabetic with a foot ulcer, radiation for the cancer patient, and laser treatments for cervical pre-cancerous lesions are profitable interventions. Building a society that facilitates health and wellness reduces profits for many influential stakeholders.
Third, public health and prevention does not create the emotional appeal that many other political topics do. Take abortion, war, or even education. These issues are emotionally charged and can be divisive. Public health does not have the same appeal and as a result, it is often overlooked. Legislators are able to make cuts in this area without the political fallout or emotional reaction.
Cutting funds for the Prevention and Public Health Fund is unfortunate. Grassroots movements and public awareness campaigns are needed to highlight the necessity of public health interventions; I believe these campaigns should be led by primary care providers. Primary care providers are respected and are leaders in building a healthy society. Getting involved at the grassroots level is the best way to show communities, states, and the nation, how important investments in public health and prevention are to our country.
Reference:
Health Affairs Policy Brief, “The Prevention and Public Health Fund,” Health Affairs, February 23, 2012
Schroeder, S., "We can do better -- Improving the Health of the American People," The New England Journal of Medicine; 2007; 357: 1221-28
Thursday, March 8, 2012
Emphasizing Primary Care in Medical Education: Utah's Primary Care Track
Medical schools across the country are implementing exciting and innovative curricular reforms to promote and encourage students to pursue primary care medicine, but the University of Utah School of Medicine is in a crowd of their own. Utah has created a primary care track for medical students interested in family medicine, pediatrics, or internal medicine. They start developing leaders in primary care as early as the first few weeks of medical school.
During the first two years of medical school, which are focused on basic science, Utah has found a way to better incorporate primary care values into their students' experience. First year students work as a medical assistant in a local clinic during their orientation month generating a better appreciation for the work that others on the medical team perform. Additionally, first year students work in a longitudinal clinic that they go to for a half day every other week. Continuity of care is a core value of all primary care, so Utah is exposing students to this important aspect of the field early. Also, during the first couple years, strong focus is put on clinical and communication skills.
Utah is alone in how they utilize the fourth year of medical school to better prepare students for their first day as a primary care intern. The curricular reform was derived from a need to make fourth year more productive and useful for students. The fourth year is broken into four components: longitudinal course, 4 week module, continuity care clinics, and teaching.
In the longitudinal component, all students in the primary care track spend a half day together, two times per month. Each longitudinal session is focused on an important issue or skill needed by primary care doctors. Some topic examples include communication, team building, ethics, public health, health reform, and health systems. The students have specific assignments during each of these sessions to tie it back into the rotation that they are currently on. For example, if a student is doing a cardiology rotation, they will have an assignment to bring in the primary care issue being discussed to that rotation. It is a way to make each fourth year rotation pertinent to primary care.
The four week module is a more intensive time to hone skills that are specifically needed by interns. They review note writing and see a lot of standardized patients to develop important technical and interpersonal skills.
The continuity care patient experience is the most exciting aspect of the primary care track. Towards the end of their third year, students recruit a panel of patients who they will track the entire year. Every time a patient on their panel has an appointment -- whether the appointment is for surgery, delivery, primary care, oncology, etc. -- the student accompanies them and serves as their health advocate. This experience shows students the inner workings of the U.S. health system firsthand, but also provides a valuable asset to patients. Having a medical professional present who knows your medical history inside and out improves care and outcomes. Kinks are still being worked out with this aspect of the track, but the idea is innovative and a very important component of their curriculum.
Lastly, the students in the primary care track have obligations to teach second year medical students. Primary care doctors need teaching skills for their patients and future medical trainees, so this is a time to develop those while reviewing important science knowledge and technical skills.
Utah is ahead of the crowd in terms of creating an innovative, primary care centered medical curriculum. It will be worth keeping tabs on how this program continues to develop.
During the first two years of medical school, which are focused on basic science, Utah has found a way to better incorporate primary care values into their students' experience. First year students work as a medical assistant in a local clinic during their orientation month generating a better appreciation for the work that others on the medical team perform. Additionally, first year students work in a longitudinal clinic that they go to for a half day every other week. Continuity of care is a core value of all primary care, so Utah is exposing students to this important aspect of the field early. Also, during the first couple years, strong focus is put on clinical and communication skills.
Utah is alone in how they utilize the fourth year of medical school to better prepare students for their first day as a primary care intern. The curricular reform was derived from a need to make fourth year more productive and useful for students. The fourth year is broken into four components: longitudinal course, 4 week module, continuity care clinics, and teaching.
In the longitudinal component, all students in the primary care track spend a half day together, two times per month. Each longitudinal session is focused on an important issue or skill needed by primary care doctors. Some topic examples include communication, team building, ethics, public health, health reform, and health systems. The students have specific assignments during each of these sessions to tie it back into the rotation that they are currently on. For example, if a student is doing a cardiology rotation, they will have an assignment to bring in the primary care issue being discussed to that rotation. It is a way to make each fourth year rotation pertinent to primary care.
The four week module is a more intensive time to hone skills that are specifically needed by interns. They review note writing and see a lot of standardized patients to develop important technical and interpersonal skills.
The continuity care patient experience is the most exciting aspect of the primary care track. Towards the end of their third year, students recruit a panel of patients who they will track the entire year. Every time a patient on their panel has an appointment -- whether the appointment is for surgery, delivery, primary care, oncology, etc. -- the student accompanies them and serves as their health advocate. This experience shows students the inner workings of the U.S. health system firsthand, but also provides a valuable asset to patients. Having a medical professional present who knows your medical history inside and out improves care and outcomes. Kinks are still being worked out with this aspect of the track, but the idea is innovative and a very important component of their curriculum.
Lastly, the students in the primary care track have obligations to teach second year medical students. Primary care doctors need teaching skills for their patients and future medical trainees, so this is a time to develop those while reviewing important science knowledge and technical skills.
Utah is ahead of the crowd in terms of creating an innovative, primary care centered medical curriculum. It will be worth keeping tabs on how this program continues to develop.
Saturday, February 25, 2012
Accountable Care Organizations: Par for the Course
Betty Jo was one of my favorite patients as a medical student. This 71 year old widow, with an obsessive zest for golf, was also one of my best teachers. It took this affable elderly woman to demonstrate the United States health system’s fragmentation before I truly understood the magnitude of the problem. She was a motivated patient who was lost in the shuffle between doctor visits. Miscommunication was the norm between my preceptor and Betty Jo’s other providers. She had 20 medications scribbled on an old piece of yellow legal paper, but nobody knew what she was actually taking, not even Betty Jo. I was embarrassed by her care which resulted in poor outcomes, deteriorating health, and multiple hospitalizations.
Like Betty Jo, over half of Medicare beneficiaries have five or more chronic diseases1. Chronic illnesses require new and innovative ways to deliver care. A 10 minute appointment slot that culminates with a blood draw and limited free samples of necessary life-saving medications represents a failure of our pre-ACA system. Running from one doctor’s appointment to the next, getting each of her diseases treated individually is proving ineffective. The quality of care is poor, costs are exponentially rising, treatment regimens are uncoordinated, medical tests are redundant, hospitalizations and emergency room visits are frequent, and the patients are unhealthy and unsatisfied with their care.
For Betty Jo and the other 47 million Medicare enrollees, Title III of the Affordable Care Act (ACA) hopes to provide an answer2. Title III establishes a shared savings program with organizations, known as Accountable Care Organizations (ACO), which will take responsibility for all aspects of Medicare patients’ care, including quality and cost. ACOs will bring together groups of doctors, other providers, and hospitals under one network3. ACOs that agree to manage all the health needs of at least 5,000 beneficiaries for no less than three years will roll out this spring 4.
The most exciting aspect of an ACO is that it will create an environment conducive to clinical innovations. ACOs will liberate providers from the chains of fee-for-service, and pay them in ways that promotes creativity and innovation in care delivery. Practices will finally step outside antiquated delivery models and start utilizing group visits, team based care, longer patient visits, and technology to maximally enhance patients’ health. Specifically, in a world where non-communicable diseases are the most salient health problem, this new model of care will integrate all components of the care delivery chain, improving health outcomes, and keeping patients, like Betty Jo, out of the hospital and on the golf course.
ACOs show promise and are being touted by some as the solution that will revolutionize health care delivery across the U.S., but I see three challenges ACOs must overcome to achieve effects of that magnitude: (1) primary care physician (PCP) shortage, (2) inaccuracy and inexperience assessing quality, and (3) inability to reach rural and other underserved populations.
The PCP shortage creates a barrier for successful implementation of ACOs. At the center of the ACO model are PCPs who are essential for providing access into the network, and then coordinating and integrating care with others in the medical neighborhood. Specialist providers are good at treating illness once the patient is already sick, but the goal of an ACO is to keep patients healthy and to reduce both specialty care and hospitalizations4. PCPs are specifically trained to provide comprehensive care focused on keeping the patient healthy. When prevention, health maintenance, and routine care fall short, they are experts at connecting patients with appropriate specialty care when needed. ACOs will ask more of PCPs, but with too few providers available, it will limit the capacity of ACOs5.
The second major challenge moving forward will be to determine what quality indicators are important and how these metrics are measured. As payment and shared savings are tied into quality control, it will be critical to ensure that the metrics accurately reflect the care being provided. A recent report from the Inspector General discusses how quality measures from electronic databases are often too blunt and are unable to provide useful information on targeted outcomes6. Quality measures must be able to tease out the direct effects that providers have on patient outcomes, but the science of measuring this will take time to fully mature. Lastly, many practices have limited or no previous experience with monitoring quality data7. For these practices, operating under new quality and cost incentives will feel like making their way in the dark.
The last major impediment to successful implementation is that ACO models will be difficult to adopt in rural health clinics (RHCs) and Federal Qualified Health Centers (FQHCs). One out of five Medicare recipients lives in a rural area and in 12 states over 50% of the Medicare population is rural8. RHCs will not have sufficient startup capital or enough patients to justify bearing financial risk for their care. Even with the subsidies and tiered risk-bearing which was negotiated last October, it is feared that the financial incentives will not be enough unless the total potential savings is increased7. FQHCs serve 1.4 million Medicare beneficiaries and face a similar situation. It will require extra incentives for them to take responsibility for the outcomes of this inherently high risk population9.
Despite these challenges, ACOs show promise for delivering better health care to patients like Betty Jo. Betty Jo’s primary care provider will finally have the time and tools he needs to coordinate and integrate care effectively and ultimately keep her healthy and out of the hospital. This will encourage clinical innovations that are patient-centered, more efficient, and higher quality; all this will cost Betty Jo, as well as the overall health system, less10. Private insurers have already shown interest in negotiating ACO-like contracts, so non-Medicare patients will benefit as well11. For Betty Jo, her future looks bright and her new biggest concern will the bogey she just got on the 18th hole.
References:
1. Accountable Care Organizations: Improving Care Coordination for People with Medicare, Healthcare.gov; November 16, 2011
2. State Health Facts, “Total Number of Medicare Beneficiaries 2011,” Kaiser Family Foundation; February 2012
3. McDonough, J., Inside National Health Reform; University of California Press; New York 2011
4. Gold, J., “ACO is the hottest three letter word in health care,” Kaiser Health News; October 21, 2011
5. Centers for Medicare and Medicaid Services website; https://www.cms.gov/ACO/, accessed February 19, 2012
6. Levinson, D., “Adverse Events in Hospitals: Methods for Identifying Events,” Department of Health and Human Services; March 2010
7. Berwick, D., “Making Good on ACO’s Promise: The Final Rule for the Medicare’s Shared Savings Program,” The New England Journal of Medicine, 365:19; November 10, 2011
8. Kaiser Family Foundation, “Percent of Medicare Beneficiaries Residing in Rural Counties, by State, 2010,” February 2012
9. MedPac, “Federally Qualified Health Centers,” MedPac Report to Congress; June 2011
10. Merlis, M., “Accountable Care Organizations,” Health Affairs; July 27, 2010
11. Fisher, E., McClellan, M., and Safran, D., “Building the Path to Accountable Care,” New England Journal of Medicine; 365: 26, December 29, 2011
Thursday, February 23, 2012
Access and the ACA: looming challenges
Expanded access to health care insurance: this promise of the Affordable Care Act (ACA) is historic as it creates a path to finally eliminate the ugly black mark on the United States as the only wealthy, developed nation without universal access to health insurance[i]. Within Title I of the law, details related to the expansion of private health insurance coverage and the regulation of the private health insurance market are laid out. In Title II, public programs including Medicaid and the Children’s Health Insurance Program are set to expand. Estimates from the Congressional Budget Office (CBO) project that 32 million uninsured Americans will gain coverage by 2019; half of them will obtain private coverage under Title I, while half will obtain coverage through the Medicaid Expansions of Title II[ii]. For a country with nearly 50 million of its people uninsured as of 2010[iii], this legislation takes a large leap forward in providing access to care.
Yet, health insurance is only one piece of the health access puzzle. While insurance reduces the economic barrier to accessing health care services, the barrier of health service availability still looms large on the horizon. Health insurance coverage is not enough to increase access to health care services, but must be coupled with an adequate supply of health care services to meet the demand of the insured. As demonstrated by the RAND Health Insurance Experiment, we can expect that as these 32 million Americans gain coverage, the demand for health care services will increase substantially, placing huge demands on our health care system[iv]. The question becomes: are we prepared to meet that demand?
Current debate around this question has focused on whether or not the physician work force, specifically, the primary care health provider work force, will be adequate to meet the new demand. Drawing on the example of Massachusetts where insurance was mandated in 2006, evidence has shown that health insurance without an adequate number and appropriate distribution of primary care physicians does not lead to health access. Since the mandate, Massachusetts has seen greater wait times for appointments with PCPs and fewer than 50% of PCPs accepting new patients[v]. This has led experts to project that with the advent on national health insurance expansion, the U.S. is on the brink of a primary care crisis. The Association of American Medical Colleges projects that the U.S. will face a shortage of approximately 21,000 PCPs by 2015[vi], while the American Academy of Family Physicians projects a shortage of 40,000 generalist physicians by 2020[vii]. While the actual number is likely to fall somewhere in between, the height of the numbers is worrisome.
Within the ACA, there are some provisions to address primary care physician workforce. These provisions include:
(1) $168 million to go towards training 500 new primary care physicians (PCP) through the creation of new residency spots by 2015,
(2) $5 million for states to create strategies to expand the primary care workforce by 10-25% over ten years to meet increased demand,
(3) $1.5 billion to strengthen the National Health Service Corps (NHSC) and to increase primary care physicians, nurse practitioners, and physician assistants by 12,000 total,
(4) Financial incentives to practice primary care in under-served areas, and financial incentives to care for Medicaid patients in 2013 and 2014.
(5) Provisions to expand the Physician Assistant (PA) and Nurse Practitioner (NP) workforce[viii].
Since health insurance without adequate health care supply does not result in greater access to care, better health outcomes, or reductions in cost, the expansion of the primary care physician workforce is vitally important to the overall success of the ACA. But will the above provisions meaningfully address this imminent problem?
The answer lies in the success of their implementation. The creation of new residency positions for primary care physicians will be helpful only if there are new physicians to fill the spots. In the last several years, family medicine and internal medicine have shown the highest unfilled residency position numbers by U.S. medical graduates. In the case of Family Medicine, 57.8% of all residency spots are filled by international medical graduates[viii]. In addition to continued reliance on international medical grads, the Federal Government is counting on the bolstered funding to the NHSC to incentivize U.S. medical students to choose primary careers in under-served areas by forgiving the loans of students who choose to enter this program. Yet, loan burden, even with debt burdens around $160,000 or higher, pales in comparison to the $3 million lifetime salary gap faced by students choosing a primary care career over a specialist career[ix]. Not to mention, years of research has supported that the choice of specialty career is influenced by multiple factors besides financial incentives, including student and institutional factors[x]. It is not at all clear that these financial incentives will be enough to induce student demand towards primary care careers.
The provisions to increase the number of practicing NP’s and PA’s will also face implementation challenges. To begin with, only one-third of PA’s currently practice within a primary care setting, limiting the effect of this legislation on the primary care shortage. While the majority of NP’s do practice in primary care settings, current estimates suggest that two NP’s are needed to cover the same workload as one PCP[xi]. Additionally, the function of NP’s is constrained by health plan and state restrictions on scope of practice. For the expansion of NP’s to contribute meaningfully to the primary care physician shortage, these constraints will need to be loosened[xii].
Finally, even if government projections are correct and the primary care workforce increases by 12,000 (a very generous estimate), this is not nearly enough to meet the projected 21,000-40,000 PCP shortage. Even more troublesome is that the impact of this shortage is likely to fall heaviest on the 16 million new Medicaid beneficiaries, due to low physician participation in Medicaid and infrequent physician practice presence in low-income communities[xiii].
The ACA is pivotal in the course of health care in the US. Yet, if the ACA is to successfully achieve the goal of expanded access, more must be done in order to bolster the primary care physician workforce. Insurance coverage without physician availability is not enough. While the above provisions are an important starting point for addressing this problem, additional new investments to strengthen the primary care workforce must become the top priority of those hoping to see the ACA succeed.
[i] OECD (2011), Government at a Glance 2011, OECD Publishing, Paris.
[ii] McDonough, John. Inside National Health Reform. University of CA Press and the Milbank Fund, 2011
[iii] United States Census Bureau, Income, Poverty and Health Insurance Coverage in the United States: 2010. Retrieved fromhttp://www.census.gov/newsroom/releases/archives/income_wealth/cb11-157.html on February 19th, 2012.
[iv] Joseph P. Newhouse and the Insurance Experiment Group. Free for All? Lessons from the RAND Health Experiment. Cambridge, Mass.: Harvard University Press, 1993,
[v] Lowry, F. Massachusetts Universal Healthcare Coverage Reveals Serious Shortage of Primary Care Physicians. www.medscape.com October 8th, 2009.
[vi] Results of the 2010 Medical School Enrollment Survey. Center for Workforce Studies. AAMC, June 2011.
[vii] AAFP Projects PCP Shortage Could Reach 40,000 By 2020. News. Robert Wood Johnson Foundation, August 17, 2009. http://www.rwjf.org/humancapital/digest.jsp?id=21508
[viii] National Resident Matching Program. AAFP 2012. http://www.aafp.org/online/en/home/residents/match.html
[ix] Fact Sheet: Creating Jobs and Increasing the Number of Primary Care Providers. www.HealthrReform.Gov. U.S. Department of Health and Human Services. Feb 20 2012.
[x] Bryan T. Vaughn, Steven R. DeVrieze, Shelby D. Reed and Kevin A. Schulman. Can we close the income and wealth gap between specialists and primary care physicians? Health Affairs, 29 no.5 (2010): 933-940.
[xi] Senf JH, Campos-Outcalt D, Kutob R. Factors related to the choice of family medicine: A reassessment and literature review. J Am Board Fam Pract. 2003 Nov-Dec;16(6):502-12.
[xii] Improving Access to Adult Primary Care in Medicaid: Exploring the Potential Role of Nurse Practitioners and Physician Assistant. Kaiser Commission on Medicaid and the uninsured. The Henry J. Kaiser Family Foundation, March 2011.
[xiii] Fact Sheet: Creating Jobs and Increasing the Number of Primary Care Providers. www.HealthrReform.Gov. U.S. Department of Health and Human Services. Feb 20 2012.
Saturday, February 18, 2012
PBS Documentary: U.S. Health System: The Good News
PBS's recent documentary on communities in the United States that are providing high quality health care at a lower cost is inspiring and worth checking out. They highlight several communities across the nation, including Grand Junction, CO, Group Health in Seattle, and physician practices in Everett, WA. Communities are doing great things, but in isolation. This documentary shows us that we are capable of providing high quality care, efficiently and cost effectively. Hopefully, medical communities across the nation will adopt practice patterns that are similarly responsive the health needs of the population.
Check out the documentary here.
BWC
Wednesday, February 8, 2012
Ezekiel Predicts the End of Insurance Companies by 2020
Ezekiel Emanuel boldly proclaims that insurance companies will be extinct by 2020 in last week's New York Times article. He believes that Accountable Care Organizations (ACO) will push them out of the market. It will be interesting to follow his prediction over the next 8 years to see if he is correct.
Emanuel explains that ACOs will eventually bear all the financial risk for patient care when they are implemented which will eliminate the need for insurance companies. ACOs, which will be composed of groups of doctors, other providers, and hospitals, will work together to provide the full range of patient care. Eventually, he sees patients paying a flat rate directly to ACOs, who, in turn, will provide all services needed. The advantage of the ACO model is that it incentivizes providers to keep the patient healthy and focus on prevention, rather than provide care only at the point of illness. Additionally, it will integrate care for the patient, creating better collaboration between different providers.
At the moment, 60% of insured citizens under age 65 in the U.S. are insured through their employer. In these cases, the financial risk falls on the employer, not the insurance company. This leaves the insurers there to help with processing claims and to provide negotiating power with hospitals and doctors. However, ACOs will charge a flat premium, which should reduce the amount of administrative work required to process and file insurance claims on a case by case basis. In situations where insurance companies take on financial risk for patients’ health – such as small businesses and individuals – they have enough market power to cherry pick healthy patients, charge high premiums, and deny patients’ claims. When ACOs start being implemented, insurance companies will be competing with ACOs for these patients. This will infuse better competition and should reduce the need for patients to hassle with insurance companies over coverage.
Emanuel also breaks down the difference between ACOs and HMOs in a very concise manner. First, ACOs and HMOs are similar such that patients are members of the organization and members pay a flat fee. In other words, payment is not done on a fee for service manner in either of these models of care. However, Emanuel emphasizes that ACOs will be local groups of providers, not large national corporations like many HMOs, so ACOs will be able to better respond to local patient needs. Also, ACOs will be financially incentivized to keep patients healthy rather than only getting paid to treat the sick. Lastly, he points to the advancements in electronic medical records as well as the science of care integration as improvements since the HMOs’ day.
Personally, I am not fully convinced that insurance companies will be extinct by 2020. It may be that I do not understand ACOs to the depth that Emanuel does. But, maybe in the end, ACOs will become large enough that they will just take over coverage responsibilities as well. Time will only tell.
BWC
Monday, February 6, 2012
Why Doesn't Pay-for-Performance Work?
Why doesn’t pay for performance work? It seems that by defining health outcomes and financially incentivizing physicians to meet those targets, we would see improved health. However, since the United Kingdom (UK) has implemented pay-for-performance incentives, the evidence that this change improves health status is negligible.
Researchers from the National Primary Care Research and Development Centre have been tracking health outcomes for asthma, diabetes, and coronary artery disease since implementing a pay-for-performance model in the UK. They found that health outcomes for asthma and diabetes improved, but only in the short run. In the long run, the rate of improvement leveled off. For heart disease, the results were even more disappointing as they did not even show improvement in the short run.
A study from the Department of Public Health Sciences, looking at intermediate outcomes of diabetes under pay-for-performance did not provide any better news. In fact, their results were not able to show a statistically significant difference in physicians’ ability to meet performance targets after rewarding physicians based off of performance.
The researchers also collected data from patients asking about perceptions of access to care, continuity of care, and the interpersonal aspects of care. The pay-for-performance method had no effect on any of these indicators either.
Performance based payment works in other fields, but for some reason it does not work in health care. This may point to the need to better define quality in health care, particularly in primary care. Maybe looking at HgA1c targets is fine on the individual level, but for population based diabetes control, this is not the answer? Perhaps, physicians are not incentivized by payment as much as economists would like us to believe? I am not sure what the problem is, but these results point us away from pay-for-performance as the silver bullet for improved quality in primary care.
BWC
References:
Stephen Campbell, et al, "Effects of Pay for Performance on the Quality of Primary Care in England," The New England Journal of Medicine 2009; 361: 368-78
Stephen Campbell, et al, "Quality of Primary Care in England with the Introduction of Pay for Performance," The New England Journal of Medicine 2007; 357: 181-190
Pooja Vaghela et al, "Population Intermediate Outcomes of Diabetes Under Pay-for-Performance Incentives in England from 2004-2008" Diabetes Care 2009; vol 32, no. 3
Researchers from the National Primary Care Research and Development Centre have been tracking health outcomes for asthma, diabetes, and coronary artery disease since implementing a pay-for-performance model in the UK. They found that health outcomes for asthma and diabetes improved, but only in the short run. In the long run, the rate of improvement leveled off. For heart disease, the results were even more disappointing as they did not even show improvement in the short run.
A study from the Department of Public Health Sciences, looking at intermediate outcomes of diabetes under pay-for-performance did not provide any better news. In fact, their results were not able to show a statistically significant difference in physicians’ ability to meet performance targets after rewarding physicians based off of performance.
The researchers also collected data from patients asking about perceptions of access to care, continuity of care, and the interpersonal aspects of care. The pay-for-performance method had no effect on any of these indicators either.
Performance based payment works in other fields, but for some reason it does not work in health care. This may point to the need to better define quality in health care, particularly in primary care. Maybe looking at HgA1c targets is fine on the individual level, but for population based diabetes control, this is not the answer? Perhaps, physicians are not incentivized by payment as much as economists would like us to believe? I am not sure what the problem is, but these results point us away from pay-for-performance as the silver bullet for improved quality in primary care.
BWC
References:
Stephen Campbell, et al, "Effects of Pay for Performance on the Quality of Primary Care in England," The New England Journal of Medicine 2009; 361: 368-78
Stephen Campbell, et al, "Quality of Primary Care in England with the Introduction of Pay for Performance," The New England Journal of Medicine 2007; 357: 181-190
Pooja Vaghela et al, "Population Intermediate Outcomes of Diabetes Under Pay-for-Performance Incentives in England from 2004-2008" Diabetes Care 2009; vol 32, no. 3
Wednesday, February 1, 2012
Public vs. Market
I am taking a class at Harvard School of Public Health this term called "Health Care Issues: Public vs. Market." It is a cumbersome title, but defines the topic and scope of the course well. Essentially it applies the debate between free markets and government intervention to the Affordable Care Act (ACA). Our first policy memo (which kind of blends into an essay in my case) was about our personal thoughts on the public vs. market debate. Are there times when government intervention in health care is necessary and if so, when and how? I offer up a few suggestions.
-------------------
We are at a significant turning point in the history of healthcare in this country. With the passage of the Affordable Care Act (ACA)in 2010 and the upcoming elections in November 2012 the debate about marketsand government in health care is intense. In this memo I will explain thebenefits of competitive markets and then explain why the health care market differs. I will finish with a discussion of the ACA and how it addresses theseissues.
Competitive markets have been the foundation of an Americaneconomy that is the largest in the world. Competition for profit spursinnovation, contains prices, and gives the consumer choice. Innovationresults when companies consistently push the envelope with new technologies,products, and production processes in an effort to expand their market share andmaximize profits. Competition alsoworks to keep prices for consumers low. Companies search for new, moreeconomical methods of production and reduce inefficiencies in their businessmodels. Southwest Airlines, for example, has repeatedly reduced operatingcosts by eliminating “frills” and shortening turnaround time between flights inorder to keep their prices competitive. Lastly, markets give the consumerchoice. In truly competitive markets, many businesses provide the same orslightly variable products from which the consumer can choose.
Health care differs from perfect markets in several ways, however. First, many view health care as a human right and believe access tohealth care should not be based on employment status or ability to pay. Second, health care is an unpredictable need and often catastrophicallyexpensive. An insurance market is a viable solution. The twoclassic problems in the health insurance market, however, are moral hazard andadverse selection. Moral hazard is the principle that after obtaininginsurance, patients will seek care they do not need, because it is free at the“point of sale.” Adverse selectionis the principle that patients know more about their state of health thaninsurance companies and therefore will buy insurance only when they need it. This leads to the third pitfall of a competitive health care market. Competitive markets assume perfectinformation. The informationasymmetry in health care is undeniable and unavoidable, both between insurancecompanies and patients (adverse selection) and between patients and theirproviders. Patients often do not know their medical needs and rely on theprovider (i.e. physician, hospital, etc) for advice, often in times ofemergency and stress. These issuescannot be addressed in a competitive market for health care and thus requiregovernment intervention.
The ACA contains solutions to many of these challenges that makesense. First, the ACA provides access for an estimated 32 of the 50million people in the US for whom the current system was failing, increasing equityin a way the market cannot. Previously, affordable health insurance was availableonly through Medicare, Medicaid, and employer-sponsored insurance, incentivizedthrough tax subsidies to companies who provide insurance for their employees. Second, companies were not mandated toprovide insurance to employees, nor individuals to carry it. This created equity and adverseselection issues, especially for the individual market. The ACA now implements a mandate with subsidiesfor persons unable to afford to buy insurance on their own. Third, the ACA places an emphasis onquality and transparency. Regulatingquality measures gives consumers more information and power to make rationaldecisions about where they will seek care. The insurance exchanges promote transparency whenindividuals are choosing a coverage plan. These are important interventions to improve information symmetry.
-------------------
MEMORANDUM
To: Speaker of the House
From: Jason Kroening-Roche
Re: Public vs. Market in Health Care Reform
Date: January 30, 2012
To: Speaker of the House
From: Jason Kroening-Roche
Re: Public vs. Market in Health Care Reform
Date: January 30, 2012
We are at a significant turning point in the history of healthcare in this country. With the passage of the Affordable Care Act (ACA)in 2010 and the upcoming elections in November 2012 the debate about marketsand government in health care is intense. In this memo I will explain thebenefits of competitive markets and then explain why the health care market differs. I will finish with a discussion of the ACA and how it addresses theseissues.
Competitive markets have been the foundation of an Americaneconomy that is the largest in the world. Competition for profit spursinnovation, contains prices, and gives the consumer choice. Innovationresults when companies consistently push the envelope with new technologies,products, and production processes in an effort to expand their market share andmaximize profits. Competition alsoworks to keep prices for consumers low. Companies search for new, moreeconomical methods of production and reduce inefficiencies in their businessmodels. Southwest Airlines, for example, has repeatedly reduced operatingcosts by eliminating “frills” and shortening turnaround time between flights inorder to keep their prices competitive. Lastly, markets give the consumerchoice. In truly competitive markets, many businesses provide the same orslightly variable products from which the consumer can choose.
Health care differs from perfect markets in several ways, however. First, many view health care as a human right and believe access tohealth care should not be based on employment status or ability to pay. Second, health care is an unpredictable need and often catastrophicallyexpensive. An insurance market is a viable solution. The twoclassic problems in the health insurance market, however, are moral hazard andadverse selection. Moral hazard is the principle that after obtaininginsurance, patients will seek care they do not need, because it is free at the“point of sale.” Adverse selectionis the principle that patients know more about their state of health thaninsurance companies and therefore will buy insurance only when they need it. This leads to the third pitfall of a competitive health care market. Competitive markets assume perfectinformation. The informationasymmetry in health care is undeniable and unavoidable, both between insurancecompanies and patients (adverse selection) and between patients and theirproviders. Patients often do not know their medical needs and rely on theprovider (i.e. physician, hospital, etc) for advice, often in times ofemergency and stress. These issuescannot be addressed in a competitive market for health care and thus requiregovernment intervention.
The ACA contains solutions to many of these challenges that makesense. First, the ACA provides access for an estimated 32 of the 50million people in the US for whom the current system was failing, increasing equityin a way the market cannot. Previously, affordable health insurance was availableonly through Medicare, Medicaid, and employer-sponsored insurance, incentivizedthrough tax subsidies to companies who provide insurance for their employees. Second, companies were not mandated toprovide insurance to employees, nor individuals to carry it. This created equity and adverseselection issues, especially for the individual market. The ACA now implements a mandate with subsidiesfor persons unable to afford to buy insurance on their own. Third, the ACA places an emphasis onquality and transparency. Regulatingquality measures gives consumers more information and power to make rationaldecisions about where they will seek care. The insurance exchanges promote transparency whenindividuals are choosing a coverage plan. These are important interventions to improve information symmetry.
Inconclusion, markets have been extremely successful in this country. However, the health care market needsgovernment intervention to correct market failures and there are many models toachieve this. Working within thecurrent system, however, the ACA does a good job ensuring greater access andequity, mitigating adverse selection, and protecting consumers from informationasymmetry. I recommend it for yoursupport.
Saturday, January 28, 2012
Why are Students Shying Away from Primary Care?
Primary care in the United States is in a state of crisis. Fewer medical school graduates than ever are choosing primary care as their specialty. The American Academy of Family Physicians (AAFP) states that there has been a 51.8 percent decrease in graduates going into primary care since 1997. With the current trajectory, this will leave the country with a shortage of 40,000 primary care physicians by 2020. Couple this with the aging baby boomer population and the system may crumble all together. It is universally accepted that primary care is the backbone of the health care system. It is these providers who serve as the gatekeepers into the system and are ultimately charged with protecting the overall health of individuals and the population.
Drs. Bach and Kocher make the argument that large medical school debt is pushing students into more lucrative fields to pay back their loans as quickly as possible. Their solution is to make medical school free, but then charge people for specialty training. They believe that this would incentivize students away from sub-specialization. As a medical student who will accumulate around $200,000 of debt to be educated (and who is married to a medical student with similar school loans), I clearly understand the financial constraints that this places. However, debt is only a portion of the entire story for why students are not choosing primary care fields. By putting all our focus on the debt issue, it will distract us from finding the real reasons why students are not going into primary care.
Medical students are not exposed to the wonderful sides of primary care medicine. In a general medical practice, the problems are often complex and the solutions are challenging, so it takes months or even years to attack the issues effectively. Students come in and out of primary care services on a month-by-month basis, so seeing any long term solutions to improving and promoting overall health is nearly impossible. Also, primary care physicians across the country are seeking innovative ways to improve patient care. This work is exciting, intellectually demanding, and extremely difficult to implement. We do not get exposed to this aspect of care because often times these projects take years to develop. Another issue is that in the academic setting, primary care is highly disrespected. This should not be that surprising considering academic centers are filled with super sub-specialists who do not fully appreciate how difficult it is to care for the whole patient, rather than a small part. Lastly, primary care, at its core, is about relationships. By being placed temporarily on a service, any relationships formed are superficial and casual.
Focusing solely on debt is a flawed solution. There are many programs for loan-forgiveness if students go into primary care fields. The debt argument looks dramatic on paper, but the real issues for why students are not going into the field are much deeper. Those are the areas on which we need to focus our attention; provide students with the chance for continuity of care, involve them in clinical innovations, and show them firsthand that the field is respectable and worth pursuing.
BWC
Response to Op-Ed: http://www.nytimes.com/2011/05/29/opinion/29bach.html?_r=2
Drs. Bach and Kocher make the argument that large medical school debt is pushing students into more lucrative fields to pay back their loans as quickly as possible. Their solution is to make medical school free, but then charge people for specialty training. They believe that this would incentivize students away from sub-specialization. As a medical student who will accumulate around $200,000 of debt to be educated (and who is married to a medical student with similar school loans), I clearly understand the financial constraints that this places. However, debt is only a portion of the entire story for why students are not choosing primary care fields. By putting all our focus on the debt issue, it will distract us from finding the real reasons why students are not going into primary care.
Medical students are not exposed to the wonderful sides of primary care medicine. In a general medical practice, the problems are often complex and the solutions are challenging, so it takes months or even years to attack the issues effectively. Students come in and out of primary care services on a month-by-month basis, so seeing any long term solutions to improving and promoting overall health is nearly impossible. Also, primary care physicians across the country are seeking innovative ways to improve patient care. This work is exciting, intellectually demanding, and extremely difficult to implement. We do not get exposed to this aspect of care because often times these projects take years to develop. Another issue is that in the academic setting, primary care is highly disrespected. This should not be that surprising considering academic centers are filled with super sub-specialists who do not fully appreciate how difficult it is to care for the whole patient, rather than a small part. Lastly, primary care, at its core, is about relationships. By being placed temporarily on a service, any relationships formed are superficial and casual.
Focusing solely on debt is a flawed solution. There are many programs for loan-forgiveness if students go into primary care fields. The debt argument looks dramatic on paper, but the real issues for why students are not going into the field are much deeper. Those are the areas on which we need to focus our attention; provide students with the chance for continuity of care, involve them in clinical innovations, and show them firsthand that the field is respectable and worth pursuing.
BWC
Response to Op-Ed: http://www.nytimes.com/2011/05/29/opinion/29bach.html?_r=2
Friday, January 20, 2012
Renegotiating Reimbursement: Good Policy or Good PR?
Yesterday Partners Health Care, Massachusetts largest health system, voluntarily disposed of its current contract with Tufts Health Plan and renegotiated a new four year agreement that is expected to lower the health reimbursements they receive by about $105 million dollars over the next four years.
This is significant. In a conversation I had with a Partners executive two months ago he shared that the Partners negotiating team often leaves their contract meetings with groups like Tufts feeling "proud" of the deals they are able to strike with health insurers. My impression was that Partners, with the largest market share of any hospital system in Massachusetts, knows it can throw its weight around and does quite willingly.
Not any more. Partners' decision to rework its contract with Tufts, following a similar renegotiation last year with Blue Cross Blue Shield that is estimated to save $240 million dollars, was likely due to the following.
- Altruism: although not likely the biggest factor, Partners CEO Gary Gotlieb did state that one reason for accepting smaller increases in reimbursements going forward is the growing burden of health care costs on families and businesses.
- Government pressure: the political environment in Massachusetts, and in many areas of the country, is such that all hospitals understand that costs must be cut voluntarily or else the government is likely to do it for them. With Massachusetts congress toying with rate setting as a way to control out of control medical costs, hospitals would rather be a part of a pre-emptive solution.
- ACOs: Partners was recently announced as one of 32 Pioneer ACOs set to begin this year. As part of the agreement, ACOs commit to generating at least 50% of their revenue from business models similar to that of the Pioneer Medicare program. This can only be accomplished through agreements with insurers, employer health plans, and/or Medicaid (called "Participation of Other Payers" in the CMS Pioneer ACO Fact Sheet). As part of Partners' new agreement with Tufts, approximately 70% of the patients in the plan will now be reimbursed via a global payment structure, shifting significant risk to Partners and forcing them to find ways to contain costs for all their patients, not only the Medicare population. This is exactly the goal of the ACO, and to the extent that Partners' participation in the Pioneer program is influencing this new agreement with Tufts, the ACO model is succeeding.
Whatever the reasons, I applaud any move by hospital systems to voluntarily forego future payment. Additionally, I applaud any move toward global payments and the taking on of risk by hospital and physician groups. However, scale must always be kept in perspective. While $105 million dollars is no small amount, with an annual budget of over $8 billion dollars and capital expenses totaling $3.2 billion dollars over 5 years, it doesn't seem like so much. Additionally, there has been little talk of where the $105 million dollars in "cuts" to Partners bottom line will come from. The hope is that money will be saved through care coordination and a focus on the high utilizers or perhaps a reduction in capital investments year over year. I imagine that if savings do not materialize, however, chronically underfunded mental health and substance abuse programs will instead be on the chopping block, and this would be an unwelcome result.
Despite my significant skepticism of the hospital market environment in Massachusetts and at the risk of being duped by what may turn out to be simply a PR move, I am encouraged that, whether it be altruism, the political environment, government policies, the market at work, or some combination of these, the system appears to be working. At least for today.
Subscribe to:
Posts (Atom)