IBM is launching what they are calling the "Primary Care Spring." At the risk of upstaging Occupy Spring they are seeking to revolutionize the way they take care of their employees by widely promulgating the Patient Centered Medical Home (PCMH). They are certainly not the first, but they represent a growing number of large insurers that have jumped on the wagon.
In a YouTube video presentation by Dr. Paul Grundy of IBM that can be found at the above link he describes 3 trends he is seeing:
1. Cost: good comprehensive coordinated patient-centered care saves money
2. Data: we can now help physicians make better clinical decisions because we now have the data needed to do so (how could he give a presentation without mentioning "Watson"?)
3. On-line asynchronous care: medical homes succeed because they allow for on-line and asynchronous care where you don't have to see your doctor to be treated and they don't have to see you to get paid. In this new information age our children will not put up with receiving care any other way.
In short, this is nothing new but it is all coming together across the country. The government, insurers, employers, providers, and patients are all recognizing that accessible, coordinated, patient-centered care really does save money and make people healthier.
You CAN have your cake and eat it too.
-JKR

Tuesday, May 1, 2012
Monday, April 30, 2012
It's the Hospitals Stupid!
Massachusetts has been leading health reform at the state level since passing far-reaching legislation in 2006 that was the blueprint for the Affordable Care Act. They are at it again. As Martyna Skowron, a colleague from Harvard School of Public Health writes, the Massachusetts House and Senate are close to releasing their versions of comprehensive payment reform legislation for the state healthcare system. What they're likely to propose may surprise you.
Much has been made of the problem of prices in our health care system. Uwe Reinhardt, back in May 2003, wrote an article in Health Affairs titled It's the Prices Stupid: Why the United States Is So Different From Other Countries. He's been writing about the issue ever since. In short, payers in the US system pay far more for the same services in absolute dollar amounts than payers in other health systems around the world.
What follows is an excerpt from the Massachusetts Attorney General's Preliminary Report on the drivers of health care costs in the state. It is titled Investigation of Health Care Cost Trends and Cost Drivers and was released last year.
Much has been made of the problem of prices in our health care system. Uwe Reinhardt, back in May 2003, wrote an article in Health Affairs titled It's the Prices Stupid: Why the United States Is So Different From Other Countries. He's been writing about the issue ever since. In short, payers in the US system pay far more for the same services in absolute dollar amounts than payers in other health systems around the world.
Why? Extending the argument one step further, as I did in this post late last year, we find ourselves at the doorstep of the hospitals who set those prices.
"We focused our investigation on contracting practices and contract prices (i.e., the prices negotiated between health insurance companies and hospitals and physicians for hospital inpatient and outpatient care, and professional services) for commercial health insurance for the period 2004 through 2008. While our investigation continues and our analysis is not final, our preliminary review has revealed serious system-wide failings in the commercial health care marketplace which, if unaddressed, imperil access to affordable, quality health care. In brief, our investigation has shown:
- Prices paid by health insurance companies to hospitals and physician groups vary significantly within the same geographic area and amongst providers offering similar levels of service.
- Price variations are not correlated to (1) quality of care, (2) the sickness or complexity of the population being served, (3) the extent to which a provider is responsible for caring for a large portion of patients on Medicare or Medicaid, or (4) whether a provider is an academic teaching or research facility. Moreover, (5) price variations are not adequately explained by differences in hospital costs of delivering similar services at similar facilities.
- Price variations are correlated to market leverage as measured by the relative market position of the hospital or provider group compared with other hospitals or provider groups within a geographic region or within a group of academic medical centers.
- Variation in total medical expenses on a per member per month basis is not correlated to the methodology used to pay for health care, with total medical expenses sometimes higher for globally paid providers than for providers paid on a fee-for- service basis.
- Price increases, not increases in utilization, caused most of the increases in health care costs during the past few years in Massachusetts.
- The commercial health care marketplace has been distorted by contracting practices that reinforce and perpetuate disparities in pricing."
Does this surprise you? In a nutshell, hospitals have been able to set high prices for their services which insurance companies must pay because hospitals possess monopolistic market share in specific health care markets. While we would hope there is more sense to the prices we pay for health care, such that we are paying more for better care, more timely care, or because we have more complex disease, this is not the case.
The question now is: what do we do about it? The free market can only help if competition is introduced into the market. Instead, hospitals have been consolidating, making the problem worse. Is it now time for the government to step in again? The Massachusetts legislature will likely unveil proposals that endorse a multi-pronged approach. The biggest prong will be encouraging global payment and setting "milestones for growth." Furthermore, they are likely to enable the state to step in if growth is not limited to these milestones. Additionally the proposal will likely include provisions to increase price transparency, ensure more competitive market behaviors, and promote further research into cost drivers and policies that encourages providers and consumers to utilize more cost-effective care.
It should be interesting and may again influence decisions made on the national stage in regards to price reform in the future.
-JKR
Monday, March 26, 2012
Supreme Court to Start Hearings on Health Reform Today
Today, the Supreme Court will begin hearings regarding the constitutionality of parts of the Affordable Care Act (ACA). The Supreme Court will hear six hours of oral arguments over the course of the next few days looking at three issues. First, they are looking at the legality of the individual mandate. Second, they will decide if this part of the law can be severed from the rest of the ACA. And three, they will hear about the constitutionality of Medicaid expansion.
Titles I and II of the ACA will reduce the number of uninsured citizens in our country through two mechanisms: required insurance by everyone and by expanding Medicaid.
Title I is the divisive individual mandate whereas every person in this country is required by law to purchase health insurance or else they face a fine. This is similar to car insurance requirements. The individual mandate, which is historically a Republican policy idea, has been controversial since the bill was passed. Economist argue that by requiring everyone to buy insurance this will broaden the risk pool thereby protecting us all financially. Additionally, by requiring health insurance, it will reduce moral hazard such that people will not seek out coverage only when they are sick or injured.
Title II expands Medicaid to cover everyone who is under 133% of the federal poverty line. It is estimated that the Medicaid expansion will result in half of the newly insured 32 million Americans.
An important aspect of the Supreme Court hearings is whether or not the ACA can stand without Titles I and/or Title II. The ACA has already benefited millions of Americans. Young adults, who make up the second largest group of uninsured Americans, are already covered. Women's health insurance premiums have been reduced equal to their male counterparts. Provisions regarding prescription drug coverage have already saved our elderly population $32 billion. Children and adults are no longer denied coverage because they have a pre-existing condition. And most importantly, as a country we have come together to reach out to our most vulnerable populations.
The hearings this week and the subsequent ruling, which is expected to come out later this spring, will be historic and will significantly impact the lives of all Americans. For the sake of our country's health and economy, I hope to see the legislation held up.
Thursday, March 22, 2012
Match Results Are In
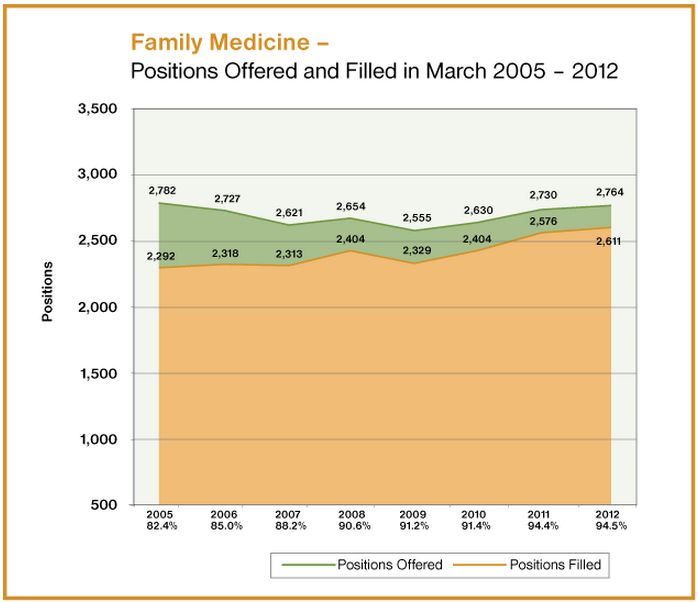 Last Friday, graduating medical students across the country received their residency match results. For the third straight year, there has been an increase in the number of students matching into family medicine. This year 94.5% of all family medicine spots were filled and the total number of U.S. grads entering the field in 2012 is 1,335. This is an increase in 18 seniors compared to 2011. Family Medicine added 34 new residency positions this year and 35 more total students (U.S. + non-U.S. grads) entered the field compared to 2011.
Last Friday, graduating medical students across the country received their residency match results. For the third straight year, there has been an increase in the number of students matching into family medicine. This year 94.5% of all family medicine spots were filled and the total number of U.S. grads entering the field in 2012 is 1,335. This is an increase in 18 seniors compared to 2011. Family Medicine added 34 new residency positions this year and 35 more total students (U.S. + non-U.S. grads) entered the field compared to 2011. Although the numbers are increasing, I hope to see further increases in the years to come. The rate of new family doctors is not keeping pace with demand and there needs to be a much larger bump in these numbers in 2013 and the following years in order to effectively serve the population's health needs.
Image from aafp.org
Wednesday, March 21, 2012
Duke's Primary Care Leadership Track
Future primary care providers will work in patient centered medical homes (PCMHs). This new model of care will be different than traditional practice models. Primary care physicians will work in inter-disciplinary teams, be expected to coordinate and integrate care with others in the medical neighborhood, and they will be held accountable for the quality of care provided to patients. Medical schools are responding by implementing programs and special tracks to prepare medical students to work in these innovative practice models.
One of the best examples nationally is Duke University School of Medicine's Primary Care Leadership Track (PCLT). Applicants to Duke's program apply specifically to the PCLT and this year alone they received well over a hundred applications. The PCLT works to develop students into national leaders in primary care.
The first year of medical school is largely the same in that students in the PCLT spend the majority of their time studying the basic sciences. At the end of their first year, they take their step 1 exams and immediately move into a longitudinal clerkship experience.
Students spend about 80 percent of their time in the outpatient setting alternating clinic days between medical practices. For example, every Monday a student will go to an internal medicine clinic, Tuesday she will go to her Family Med Clinic, Psychiatry on Wednesday, and Pediatrics on Thursday. This provides the students with continuity of care within each of the core disciplines and gives them a chance to follow their patients' care over the course of a year.
Students also are assigned to a panel of about 20 patients who they follow throughout the entire year. Every time one of the patients in their panel has a medical appointment, surgery, emergency department visit, or baby delivery, the student is expected to be there with the patient. This provides students with the unique insight of how patients flow through the medical system.
Within the PCLT curriculum, students go through a PCMH mini-course. The mini-course is designed to teach students the core values of primary care and PCMHs. Students are then engaging in medical practices who are working towards PCMH accreditation by taking on an innovation projects. A good example of a project is when one student worked with a clinic to meet phone call back goals. The student tracked the average length of time it took the clinic to call their patients back and then he worked with the clinic to shorten the interval. Other projects have looked at follow up rates and length of time from the point of hospital discharge, quality metrics for diabetic patients, and rate of specialist to primary care provider communication after the patient sees their specialist physician.
Engaging students in innovation projects is developing strong leadership skills and showing students the inner workings of this new model of care. Students will be ahead of their peers once they start practicing as they will have real life experience in improving practice models which are truly patient-centered.
Duke's focus on primary care is inspiring and they are setting the bar for preparing and producing future leaders in primary care medicine.
Friday, March 9, 2012
Prevention and Public Health Fund Gets Cut
On February 22, 2012, President Obama signed legislation to cut funding from the Prevention and Public Health Fund. This fund was created by the Affordable Care Act (ACA) and invested $15 billion over 10 years to prevent disease and promote wellness in our society. This was a major advancement in U.S. health policy which shifted focus on creating a healthy and productive society rather than one that only reacts to disease once patients are already ill.
Prevention and public health are frequently the first place to start enacting cuts, but this is a huge mistake. Most diseases and causes of death in the U.S. are preventable, yet we continue to turn our backs on efforts to stop disease, illness, injury, and even death before they develop. When we have an unhealthy society, this affects many sectors of our economy as sick or injured workers are not as productive as they could be. Additionally, by continuing to only invest at the end of the line, care is reactionary and costly for the patients.
I think three primary reasons explain why investments in public health and prevention are often overlooked. First, people do not understand what public health is. It is more than just responding to infectious disease outbreaks or tracking influenza strains. Public health makes sure that the food we eat is sanitary, the air we breathe is clean, and that our roads are safe to drive on. Nearly every facet of our lives places us in danger, but public health professionals seek to minimize risks. Most public health interventions are inconspicuous and out of the public eye, so it is not surprising that political will for public health initiatives is minimal.
Second, prevention does not make anyone any money. Health care is big business these days and bottom lines for those in the health industry only decrease when people are healthy. Money comes at the end of the line: surgery for the diabetic with a foot ulcer, radiation for the cancer patient, and laser treatments for cervical pre-cancerous lesions are profitable interventions. Building a society that facilitates health and wellness reduces profits for many influential stakeholders.
Third, public health and prevention does not create the emotional appeal that many other political topics do. Take abortion, war, or even education. These issues are emotionally charged and can be divisive. Public health does not have the same appeal and as a result, it is often overlooked. Legislators are able to make cuts in this area without the political fallout or emotional reaction.
Cutting funds for the Prevention and Public Health Fund is unfortunate. Grassroots movements and public awareness campaigns are needed to highlight the necessity of public health interventions; I believe these campaigns should be led by primary care providers. Primary care providers are respected and are leaders in building a healthy society. Getting involved at the grassroots level is the best way to show communities, states, and the nation, how important investments in public health and prevention are to our country.
Reference:
Health Affairs Policy Brief, “The Prevention and Public Health Fund,” Health Affairs, February 23, 2012
Schroeder, S., "We can do better -- Improving the Health of the American People," The New England Journal of Medicine; 2007; 357: 1221-28
Thursday, March 8, 2012
Emphasizing Primary Care in Medical Education: Utah's Primary Care Track
Medical schools across the country are implementing exciting and innovative curricular reforms to promote and encourage students to pursue primary care medicine, but the University of Utah School of Medicine is in a crowd of their own. Utah has created a primary care track for medical students interested in family medicine, pediatrics, or internal medicine. They start developing leaders in primary care as early as the first few weeks of medical school.
During the first two years of medical school, which are focused on basic science, Utah has found a way to better incorporate primary care values into their students' experience. First year students work as a medical assistant in a local clinic during their orientation month generating a better appreciation for the work that others on the medical team perform. Additionally, first year students work in a longitudinal clinic that they go to for a half day every other week. Continuity of care is a core value of all primary care, so Utah is exposing students to this important aspect of the field early. Also, during the first couple years, strong focus is put on clinical and communication skills.
Utah is alone in how they utilize the fourth year of medical school to better prepare students for their first day as a primary care intern. The curricular reform was derived from a need to make fourth year more productive and useful for students. The fourth year is broken into four components: longitudinal course, 4 week module, continuity care clinics, and teaching.
In the longitudinal component, all students in the primary care track spend a half day together, two times per month. Each longitudinal session is focused on an important issue or skill needed by primary care doctors. Some topic examples include communication, team building, ethics, public health, health reform, and health systems. The students have specific assignments during each of these sessions to tie it back into the rotation that they are currently on. For example, if a student is doing a cardiology rotation, they will have an assignment to bring in the primary care issue being discussed to that rotation. It is a way to make each fourth year rotation pertinent to primary care.
The four week module is a more intensive time to hone skills that are specifically needed by interns. They review note writing and see a lot of standardized patients to develop important technical and interpersonal skills.
The continuity care patient experience is the most exciting aspect of the primary care track. Towards the end of their third year, students recruit a panel of patients who they will track the entire year. Every time a patient on their panel has an appointment -- whether the appointment is for surgery, delivery, primary care, oncology, etc. -- the student accompanies them and serves as their health advocate. This experience shows students the inner workings of the U.S. health system firsthand, but also provides a valuable asset to patients. Having a medical professional present who knows your medical history inside and out improves care and outcomes. Kinks are still being worked out with this aspect of the track, but the idea is innovative and a very important component of their curriculum.
Lastly, the students in the primary care track have obligations to teach second year medical students. Primary care doctors need teaching skills for their patients and future medical trainees, so this is a time to develop those while reviewing important science knowledge and technical skills.
Utah is ahead of the crowd in terms of creating an innovative, primary care centered medical curriculum. It will be worth keeping tabs on how this program continues to develop.
During the first two years of medical school, which are focused on basic science, Utah has found a way to better incorporate primary care values into their students' experience. First year students work as a medical assistant in a local clinic during their orientation month generating a better appreciation for the work that others on the medical team perform. Additionally, first year students work in a longitudinal clinic that they go to for a half day every other week. Continuity of care is a core value of all primary care, so Utah is exposing students to this important aspect of the field early. Also, during the first couple years, strong focus is put on clinical and communication skills.
Utah is alone in how they utilize the fourth year of medical school to better prepare students for their first day as a primary care intern. The curricular reform was derived from a need to make fourth year more productive and useful for students. The fourth year is broken into four components: longitudinal course, 4 week module, continuity care clinics, and teaching.
In the longitudinal component, all students in the primary care track spend a half day together, two times per month. Each longitudinal session is focused on an important issue or skill needed by primary care doctors. Some topic examples include communication, team building, ethics, public health, health reform, and health systems. The students have specific assignments during each of these sessions to tie it back into the rotation that they are currently on. For example, if a student is doing a cardiology rotation, they will have an assignment to bring in the primary care issue being discussed to that rotation. It is a way to make each fourth year rotation pertinent to primary care.
The four week module is a more intensive time to hone skills that are specifically needed by interns. They review note writing and see a lot of standardized patients to develop important technical and interpersonal skills.
The continuity care patient experience is the most exciting aspect of the primary care track. Towards the end of their third year, students recruit a panel of patients who they will track the entire year. Every time a patient on their panel has an appointment -- whether the appointment is for surgery, delivery, primary care, oncology, etc. -- the student accompanies them and serves as their health advocate. This experience shows students the inner workings of the U.S. health system firsthand, but also provides a valuable asset to patients. Having a medical professional present who knows your medical history inside and out improves care and outcomes. Kinks are still being worked out with this aspect of the track, but the idea is innovative and a very important component of their curriculum.
Lastly, the students in the primary care track have obligations to teach second year medical students. Primary care doctors need teaching skills for their patients and future medical trainees, so this is a time to develop those while reviewing important science knowledge and technical skills.
Utah is ahead of the crowd in terms of creating an innovative, primary care centered medical curriculum. It will be worth keeping tabs on how this program continues to develop.
Subscribe to:
Posts (Atom)